
[Disclaimer: I am an employee of Celgene. The views reported here are my own.]
I presented at the PharmacoGenomics Research Network (PGRN) portion of the 2018 ASHG meeting (link to my slides here). A major theme from my talk was that precision medicine holds promise for advancing novel therapies, but that implementation of pharmacogenomics (PGx) will happen by design not by accident. Here is what I mean – and why our health care systems need to build for this future state today.
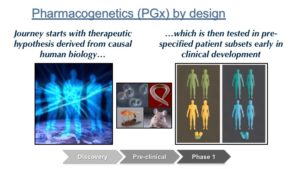
PGx by design – PGx by design starts at the very beginning of the drug discovery journey, when the choice is made to develop a therapeutic molecule against a target or a pathway. A precision medicine hypothesis is carried forward into the design of a therapeutic molecule (“matching modality with mechanism”), pre-clinical biomarkers to measure pharmacodynamic responses, and early proof-of-concept clinical studies in defined patient subsets. Late-stage clinical development is performed in these patient subsets, and regulatory approval is obtained with a label that defines this patient subset. Health care systems will essentially be required to incorporate precision medicine into patient care.
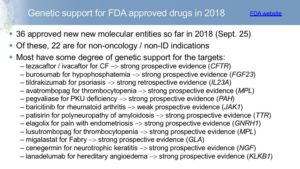
There are emerging examples of PGx by design. Indeed, there are an increasing number of FDA approvals that fit with the PGx by design model (see figure below). Most are for rare diseases, where a detailed understanding of molecular mechanism helps guide all stages of drug R&D.
PGx by accident – In contrast, “PGx by accident” happens for a therapy that was developed without a pre-defined patient segmentation hypothesis at the start of the drug development journey. Then, through germline genotyping, genomic profiling or another ‘omics technology, patients more likely to respond to the drug or those who suffer an adverse drug event (ADE) will be identified. Maybe this unexpected discovery happens during clinical development or maybe this happens post-regulatory approval. Either way, PGx profiling will then be used in the real world to practice precision medicine.
While there are examples of such – with excellent talks by Munir Pirmohamed (University of Liverpool; slide here) and Elizabeth Phillips (Vanderbilt University Medical Center) highlighting examples of severe immune-mediated ADEs (review articles here, here) – these examples are relatively few and far between, given the total number of approved drugs (see here for 2016 Nature Reviews Genetics by Matt Nelson and colleagues).
There are important implications of the “PGx by design” model.
(1) The tipping point for precision medicine is a few years away. If PGx by design is the model by which precision medicine ultimately takes root, then there will likely be a period of 5-10 years when PGx has limited impact on routine patient care. While there are an increasing number of FDA approvals that fit with the PGx by design model (see figure above), most are for rare diseases. As more PGx by design therapies are approved for common diseases, then infrastructure will emerge that enables the proper implementation of PGx within health care systems.
(2) Health care systems need to anticipate this future state…today. But even if you agree with me that routine precision medicine is several years away, health care systems need to anticipate this future state today, as the infrastructure required is substantial (see here and here). For example, consider the infrastructure required to return genetic results to patients: (a) patient consent for genetic testing; (b) GWAS genotyping for polygenic risk scores (see Nature Medicine editorial here, and Nature editorial here) and exome sequencing for rare variants; (c) delivery of results to physician; (d) interpret findings for patients; (e) clinical implementation of actionable results; and (f) electronic notification systems that alert physicians of actionable genetic results over time. Towards this end, implementation of actionable pharmacogenetic results is a good way to build the infrastructure, as highlighted throughout the PGRN-ASHG session.
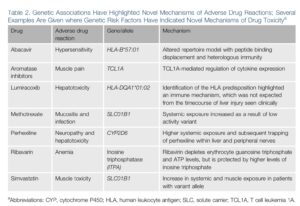
(3) PGx by accident is still important. Even though I believe that most precision medicine will happen by design, we should not stop searching for the unexpected. Many of the biological mechanisms for actionable pharmacogenetic discoveries could not have been predicted in advance (see Table below taken from this review). Thus, routine genotyping should be part of most clinical trials to search for large effect size variants that predict treatment response or adverse events (see 2014 blog on a related topic here).
(4) PGx by design may address the attrition problem in drug development. There is ample evidence that human genetics increases probability of success by at least 2-fold (see Matt Nelson slide deck here, my summary here). Thus, PGx by design has the added benefit of addressing what I refer to as the “attrition problem” in drug discovery and development (see introductory slides from my PGRN-ASHG talk).
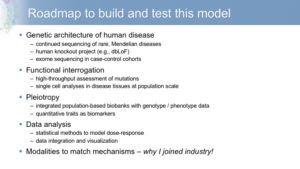
(5) There are emerging resources to help start this journey. In my PGRN-ASHG talk, I highlighted two emerging resources: Mendelian randomization and Phenome-Wide Association Studies (PheWAS). As an example of the latter, Dorothee Diogo, Heiko Runz and colleagues recently published a PheWAS on ~800,000 individuals (see Nature Communications article here). There are several new eQTL datasets from @soumya_boston (here) and @LudeFranke (here), the latter of which includes analyses in blood from 31,684 individuals through the eQTLGen Consortium. In his ASHG presentation, Eric Lander outlined other emerging resources required to start this journey, including deep sequencing of patients, cell-specific eQTLs, and efficient genome editing of variants in relevant cell types (see @skathire tweet here). I offered a high-level roadmap in my PGRN-ASHG presentation (see figure below).
(6) Oncology is leading the way. I often ignore oncology from discussions on this blog. And this “PGx by design” model is no exception! But the infrastructure to do precision oncology is evolving rapidly – and will likely set the stage for other disease areas (see here for Nature Reviews Drug Discovery article on “Trends in the global immuno-oncology landscape“). An example highlighted at the PGRN-ASHG meeting was anti-PD1 therapy approved in a subset of patients with somatic mutations due to mismatch-repair defects (see NEJM article here). Another example was published this week in NEJM, “Classification and Personalized Prognosis in Myeloproliferative Neoplasms” (here).
In conclusion, I am a firm believer that the start of every drug discovery and development journey should start with a precision medicine hypothesis. Moreover, as these hypotheses become part of the fabric of drug R&D, PGx will emerge by design rather than by accident, much in the way that the topiary sculptures were designed on the shores of Lake Waban (see figure below and history lesson here). While that journey will take time, and while the tipping point is not yet here, health care systems need to prepare for that inevitable state today.
