[I am an employee of Celgene. All views expressed here are my own.]
What is the clinical significance of residing within the tail of a distribution for disease risk? A new study published in Nature Genetics uses a composite polygenic score to measure extremes of genetic risk(see original article here). The authors make the bold statement: “it is time to contemplate the inclusion of polygenic risk prediction in clinical care”. In this plengegen.com blog, I briefly review the paper, frame the impact of the study in terms of “long tails”, and propose how genetic tails may be used as part of a healthcare system reimagined.
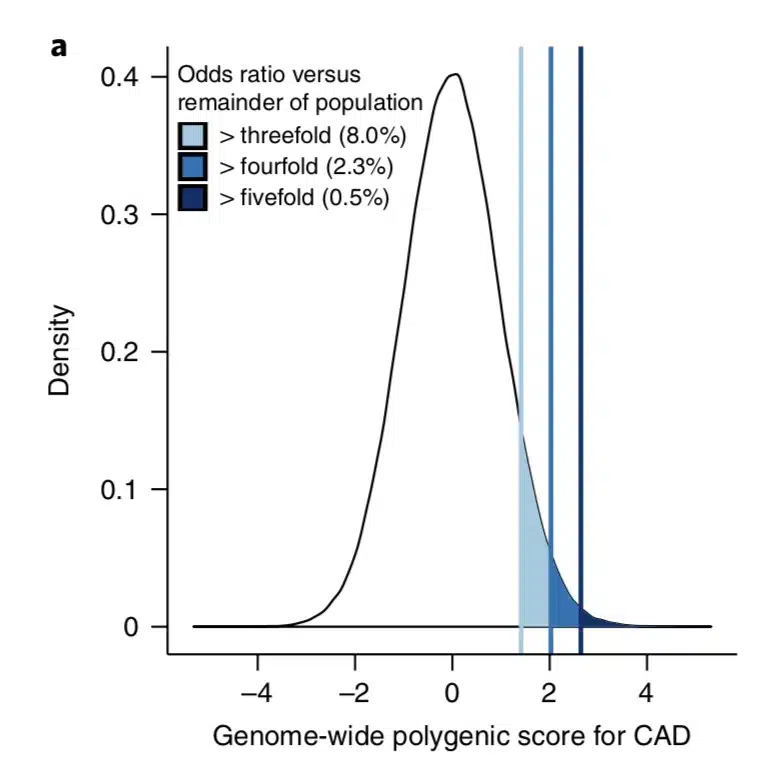
The premise of the paper is that a genome-wide polygenic score (GPS) – a composite genetic test that includes thousands and sometimes millions of genetic variants – can identify a small number of individuals from the general population that have an elevated risk. The study applies polygenic risk scores to five common diseases but spends most attention to coronary artery disease (CAD). For each disease, the increase in risk is approximately 3- to 5-fold higher among individuals at the extreme of the polygenic tail compared to those in the general population – see Figure 2a (and below) for CAD, where ~8% of the general population is at a 3-fold increase in risk based on a polygenic risk score.…
As readers of my blog know, I am a strong supporter of a disciplined R&D model that focuses on: picking targets based on causal human biology (e.g., genetics); developing molecules that therapeutically recapitulate causal human biology; deploying pharmacodynamic biomarkers that also recapitulate causal human biology; and conducting small clinical proof-of-concept studies to quickly test therapeutic hypotheses (see Figure below).As such, I am constantly on the look-out for literature or news reports to support / refute this model.Each week, I cryptically tweet these reports, and occasionally – like this week – I have the time and energy to write-up the reports in a coherent framework.
Of course, this model is not so easy to follow in the real-world as has been pointed out nicely by Derek Lowe and others (see here).A nice blog this week by Keith Robison (Warp Drive Bio) highlights why drug R&D is so hard.
Here are the studies or news reports from this week that support this model.
(1) Picking targets based on causal human biology: I am a proponent of an “allelic series” model for target identification. Here are a couple of published reports that fit with this model.…
Like many, I waited with bated breath for results of the anti-PCSK9 (evolocumab) FOURIER cardiovascular outcome study last week. There have been many interesting commentaries written on the findings.A few of my favorites are listed here (Matthew Herper), here (David Grainger), here (Derek Lowe), and here (Larry Husten), amongst others, with summaries provided at the end of this blog.Most of these articles focused on clinical risk reduction vs. what was predicted for cardiovascular outcome, as well as whether payers will cover the cost of the drugs.These are incredibly important topics, and I won’t comment on them further here, other than to say that the debate is now about who should get the drug and how much it should cost.
In this blog, I want to emphasize key points that pertain to human genetics and drug discovery.And make no mistake: the anti-PCSK9 story and FOURIER clinical trial outcome is a triumph for genetics and drug discovery. This message seems to be getting muddled, however, given the current cost of evolocumab and the observation that cardiovascular risk reduction was less than expected, based on predictions from a 2005 study published by Cholesterol Treatment Trialists (CTT) (see Lancet study here).…
Here are my thoughts on the Discussion Paper by Bernard H. Munos and John J. Orloff, “Disruptive Innovation and Transformation of the Drug Discovery and Development Enterprise” (download pdf here). This blog won’t make much sense if read out-of-context. Thus, I recommend reading the Discussion Paper itself, and using this blog as a companion guide at the completion of each section.
[Disclaimer: I am a Merck/MSD employee. The opinions I am expressing are my own and do not necessarily represent the position of my employer.]
STRENGTHS AND WEAKNESSES OF THE CURRENT INDUSTRY MODEL
In the near-term (10-years), I suspect that the pharma model of late development and commercialization will likely persist, as the cost and complexity of getting a drug approved is difficult by other mechanisms. Over time, however, new ways of performing late-stage trials will likely evolve. Drugs that are today in the early R&D pipeline will drive this evolution. If drugs look like they do today, dominated by small molecules and biologics with high probability of failure in Phase II/III, then the current model will likely continue with incremental improvements in efficiency. However, if new therapeutic modalities emerge (CRISPR, mRNA, microbiome, etc) and/or the probability of success in Phase II/III improves substantially, then the model of late development and commercialization will be forced to evolve, too.…
It is not uncommon that I am asked the following question during public talks: “Does innovation happen in large pharmaceutical companies?” Sometimes, the question is just a critical comment, disguised as a question: “Large pharma does not innovate, they just conduct clinical trials and drive up the cost of drugs. Right?” Other times the questions are more thoughtful: “As an academic, I don’t see what happens in industry. Can you describe examples of innovation driven out of large pharma?”
[Disclaimer: I am a Merck/MSD employee. The opinions I am expressing are my own and do not necessarily represent the position of my employer.]
At the risk of sounding defensive, here are some answers to the “pharma innovation” question. I know there are many more, and I invite readers to share their examples. Admittedly, the examples are biased towards examples at Merck, but that is just because I know these examples better.
First, the past couple of weeks have been particularly good for industry scientists. These recent examples provide objective evidence to answer the pharma innovation question.
(a) 2015 Nobel Prizein Physiology or Medicine. Former Merck scientist Dr. William Campbell was awarded the Nobel Prize for the discovery of an antiparasitic agent used to treat river blindness in places like Latin America, Africa and Yemen.…
If you could pick three innovations that would revolutionize drug discovery in the next 10-20 years, what would they be?
I found myself thinking about this question during a recent family vacation to Italy. I was visiting the Galileo Museum, marveling at the state of knowledge during the 1400-1600’s. The debate over planetary orbits seem so obvious now, but the disagreement between church and science led to Galileo’s imprisonment in 1633.
So what is it today that will seem so obvious to our children and grandchildren…and generations beyond? Let me offer a few ideas related to drug discovery, and hope that others will add their own. I am not sure if my ideas are grounded in reality, but that is part of the fun of the game. In addition, “The best way to predict the future is to invent it.”
To start, let me remind readers of this blog that I believe that the three major challenges to efficient drug discovery are picking the right targets, developing the right biomarkers to enable proof-of-concept (POC) studies, and testing therapeutic hypotheses in humans as quickly and safely as possible. Thus, the future needs to address these three challenges.
My overly simplistic vision of the way to transform drug discovery is to (1) pick targets based on causal human biology (e.g., experiments of nature, especially human genetics), (2) develop drugs that recapitulate the biology of the human experiments of nature (e.g., therapeutic inhibitors of proteins), (3) develop biomarkers that measure target modulation in humans, and (4) test therapeutic hypotheses in humans as safely and efficiently as possible.
Thus, one of my favorite themes is “causal human biology”. The word “causal” is key: it means that there is clear evidence between the cause-effect relationship of target perturbation in humans and a desired effect on human physiology. Human genetics represent one way to get at causal human biology, and in my last blog I highlighted recent examples outside of human genetics.
I am constantly scanning the literature to find examples that support or refute this model, as I predict that a discipline portfolio of projects based on causal human biology will be more successful than past efforts by the pharmaceutical industry.
This week I have selected two articles on genetics/genomics in drug discovery that provide further support of this model. [Disclaimer: the first study was funded by Merck, my employer.]…
Genetics can guide the first phase of drug development (identifying drug targets, see here ) as well as late phase clinical trials (e.g., patient segmentation for response/non-responder status, see here ). But is there a convergence between the two areas, or pharmaco-convergence (a term I just made up!)? And are there advantages to a program anchored at both ends in human genetics?
Consider the following two hypothetical examples.
(1) Human genetics identifies loss-of-function (LOF) mutations that protect from disease. The same LOF mutation is associated with an intermediate biomarker, but is not associated with other phenotypes that might be considered adverse drug events. A drug is developed that mimics the effect of the mutation; that is, a drug is developed that inhibits the protein product of the gene. In early mechanistic studies, the drug is shown to influence the intermediate biomarker in a way that is consistent to that predicted by the LOF-protective mutations. Further, because functional studies of the LOF-protective mutations provide insight into relevant biological pathways in humans (e.g., a gene expression signature that correlates with mutation carrier status), additional information is known about genomic signatures of those who carry the LOF-protective mutations (which mimics drug exposure) compared to those who do not carry the LOF-protective mutations (which mimics those who are not exposed to drug).…







{kind=link}
{kind=link}
{kind=link}
{kind=link}